Even more knowledge


Guided implant surgery uses 3‑D‑printed, tooth‑supported surgical guides that translate a virtual plan into the mouth with sub‑millimeter precision. By anchoring the guide to the dentition and employing fixed drill sleeves (or sleeve‑free designs), the drill cannot deviate, keeping the osteotomy at least 2 mm away from nerves, sinuses and adjacent roots, which dramatically lowers the risk of nerve injury or sinus perforation. The pre‑planned trajectory also aligns the implant with the intended prosthetic emergence, ensuring optimal angulation for crown esthetics and function. Because the guide eliminates guesswork, drilling and implant seating can be completed in 10–15 minutes, cutting chair time and allowing flapless, minimally invasive approaches that reduce postoperative swelling, pain and recovery time. Patients also benefit from a workflow that reduces the need for try‑ins and radiographs, enhancing comfort and safety.

The guided‑implant workflow begins with a CBCT scan that captures bone anatomy and an intra‑oral scanner that records the dentition. Merging these datasets in virtual implant‑planning software (e.g., 3Shape Implant Studio, Exocad) creates a prosthetically driven plan that defines implant depth, angulation, and safety margins. The finalized STL file is sent to an additive‑manufacturing unit where SLA or DLP printers fabricate a tooth‑supported surgical guide. Materials such as Formlabs Surgical Guide Resin or SprintRay Surgical Guide 2 are biocompatible, autoclavable, and printed at layer heights of 50–100 µm for high dimensional stability. Post‑processing includes support removal, resin cleaning, UV curing, and autoclaving at 134 °C for five minutes, after which the guide is verified intra‑orally for passive fit and anchor‑pin stability before surgery.
How big is the dental 3D printing market? The global market was valued at US $4.89 billion in 2025 and is projected to reach US $26.73 billion by 2033 (CAGR ≈ 23.3 %). The United States accounts for 38.6 % of revenue, with a 2025 size of US $1.56 billion.
What is the use of 3D printing in dentistry? It enables rapid, patient‑specific fabrication of restorations (crowns, bridges, dentures), orthodontic appliances, surgical guides, and implant abutments, reducing production time, cost, and clinical errors while supporting personalized, high‑precision care.
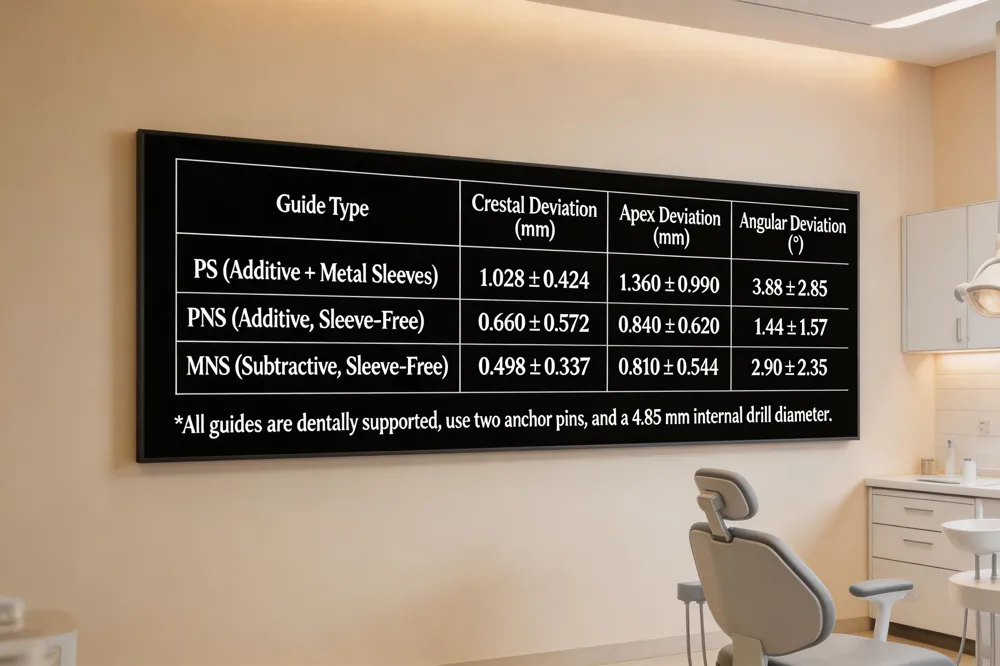 The recent in‑vitro study compared three guide designs: additive‑manufactured guides with metal sleeves (PS), additive‑manufactured sleeve‑free guides (PNS), and subtractive‑manufactured sleeve‑free guides (MNS). All were dentally supported, anchored with two pins, and used a 4.85 mm internal drilling diameter. Crestal deviation was lowest for the MNS group (0.498 ± 0.337 mm), followed by PNS (0.660 ± 0.572 mm) and PS (1.028 ± 0.424 mm). Apex deviation followed the same pattern (MNS 0.810 ± 0.544 mm; PNS 0.840 ± 0.620 mm; PS 1.360 ± 0.990 mm). Angular deviation, however, was smallest in the PNS group (1.44° ± 1.57°) and significantly larger in MNS (2.90° ± 2.35°) and PS (3.88° ± 2.85°). These results show that sleeve‑free designs consistently outperform metal‑sleeved guides in linear accuracy, while additive‑printed, sleeve‑free guides achieve the best angular control.
What I wish I knew before dental implants? I wish I’d known that the entire implant process can take weeks to months, as bone healing and osseointegration require patience for lasting stability. I also didn’t realize how much bone health matters; insufficient bone density may require grafts or other preparatory procedures before implants can be placed. The upfront cost may seem high, but when viewed over decades it often proves more cost‑effective than alternatives that need frequent repairs. Daily care is simple—just brush, floss, and keep regular dental visits—yet consistency is crucial for long‑term success. Finally, choosing an experienced provider who clearly explains each step makes the journey far less stressful and more rewarding.
How much does an implant guide cost? In the United States, a custom 3‑D‑printed implant surgical guide typically starts at about $150 for a single‑tooth case and can rise to $300‑$600 or more for multi‑unit or full‑arch treatments, depending on case complexity, CBCT integration, and planning time. Most labs charge a planning fee of $150‑$350 plus a printing fee of $145‑$265, resulting in total costs of roughly $295‑$575 for one‑to‑six‑unit guides. Practices that use in‑house CAD/CAM may see slightly lower fees, while external providers often bundle the guide with the surgical kit. Patients should ask their dentist for a detailed quote that reflects the specific treatment plan and any insurance coverage.
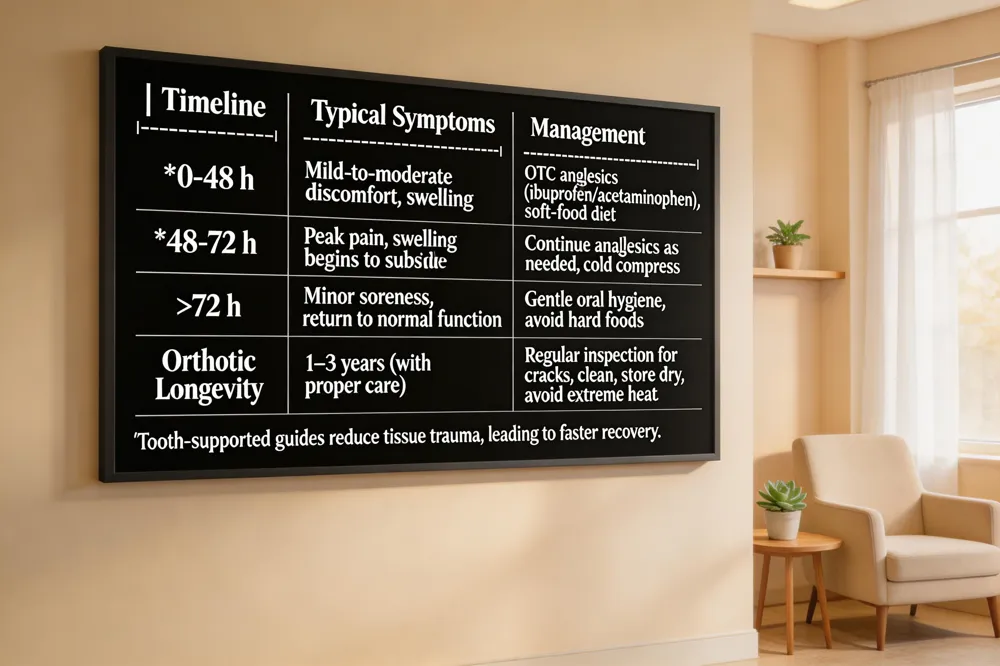 Guided implant surgery with 3D‑printed surgical guides shortens chair time and often eliminates flap elevation, which translates into less postoperative swelling and a quicker return to normal function. Most patients report mild to moderate discomfort that peaks in the first 48‑72 hours and can be managed with over‑the‑counter analgesics and a soft‑food diet. The precise, tooth‑supported guides keep the drill stable, minimizing tissue trauma and reducing the need for extensive irrigation, which further less intra‑operative heat and postoperative soreness.
What's the most painful part of a dental implant? The recovery period—especially the first two to three days after surgery—is usually the most uncomfortable phase. The surgical site may feel sore, swollen, and tender as bone and soft tissue heal, but the implant placement itself is performed under local anesthesia and is not painful.
How long do 3D‑printed orthotics last? With proper care, 3D‑printed orthotics typically last 1–3 years. Durable, biocompatible resins or TPU filaments retain their shape and cushioning longer than softer blends, while regular cleaning, dry storage, and avoiding extreme temperatures help extend service life. Inspect for cracks or loss of fit to know when replacement is needed.
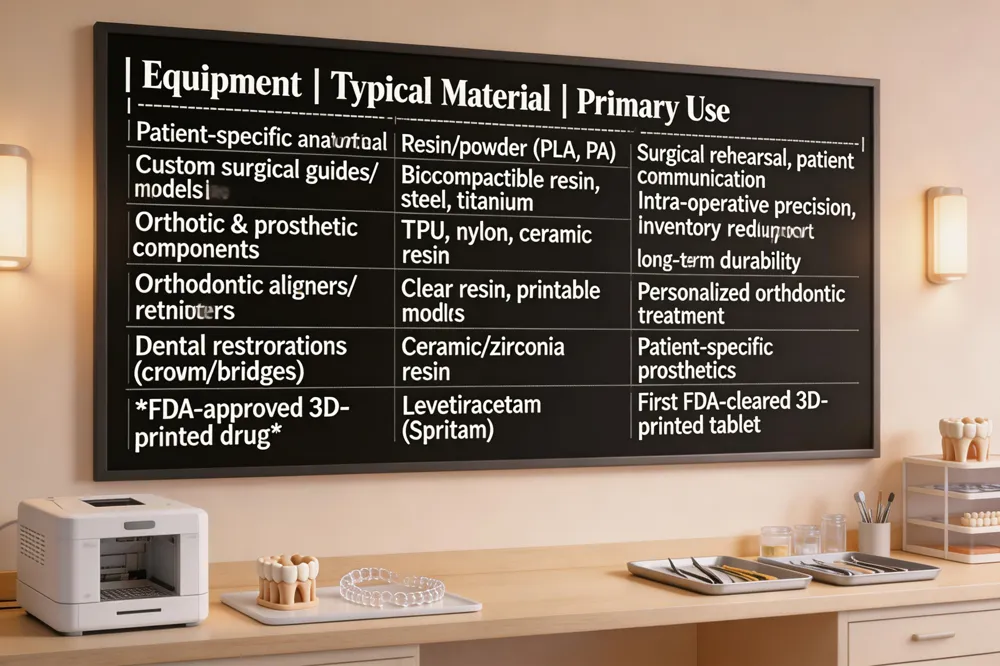
3D printing now extends far beyond dental surgical guides. Patient‑specific anatomical models—created from CBCT or MRI data—are printed in resin or powder‑based materials to let surgeons rehearse complex procedures, practice osteotomies, and improve communication with patients. Custom surgical instruments and prosthetic components, such as patient‑matched drilling jigs, orthopedic fixation plates, and even implant abutments, are fabricated on demand using biocompatible, sterilizable resins or metal powders, delivering precise fit and reducing inventory costs. In dentistry, the same workflow produces temporary crowns, permanent bridges, and complete dentures with ceramic‑filled resins, while orthodontic aligner trays, retainers, and custom brackets are molded from printed molds for rapid, personalized treatment.
What medical equipment can be 3D printed? Surgical guides, splints, patient‑specific anatomical models, custom surgical instruments, prosthetic components, orthodontic appliances, and dental restorations are routinely printed for pre‑operative planning and intra‑operative use.
What is the FDA‑approved 3D‑printed tablet? Levetiracetam, marketed as Spritam, became the first 3D‑printed drug cleared by the FDA, demonstrating the technology’s potential for complex, dose‑customized medicines.
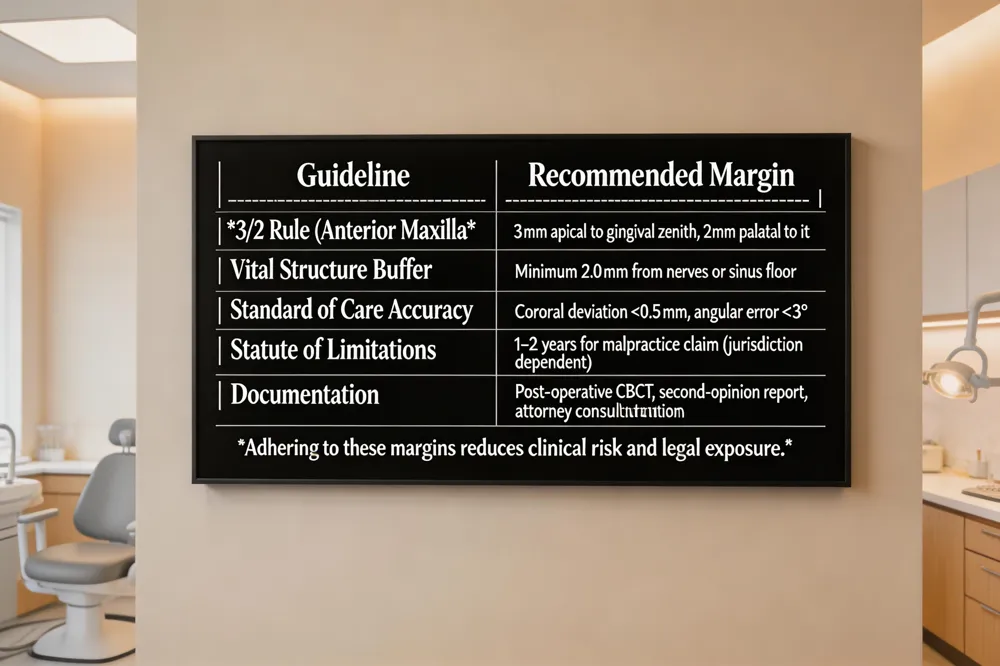 Standard of care in implant dentistry requires that the clinician translate a digitally planned trajectory into the mouth with a predictable level of accuracy. 3D‑printed surgical guides—whether additive or subtractive—have been shown to keep coronal deviations below 0.5 mm and angular errors under 3°, thereby meeting the legal expectation of “reasonable accuracy.” When a placed ends up outside the planned position, it can constitute a breach of that standard, opening the door to dental‑malpractice claims. A patient must obtain a second opinion, document the deviation (often with post‑operative CBCT), and consult an attorney within the jurisdiction’s statute of limitations, typically one to two years.
The “3/2 rule” for the anterior maxilla advises that the implant platform be placed 3 mm apical to the intended gingival zenith and 2 mm palatal to it. This guideline helps clinicians decide whether bone grafting or soft‑tissue augmentation is needed and provides a measurable safety margin.
Safety margins are critical when vital structures are nearby. Dynamic navigation studies recommend a minimum 2.0 mm buffer from nerves or sinus floors, and static guide protocols often embed safety‑zone alerts in planning software. By respecting these margins and using accurate, sleeve‑free, 3D‑printed guides, clinicians protect patients from nerve injury, sinus perforation, and the subsequent legal and health consequences of a misplaced implant.

The 50‑40‑30 rule is a classic smile‑design guideline that dictates the apparent width relationships of the anterior teeth. When a patient smiles, the central incisors should occupy roughly 50 % of the total smile width, the central‑to‑lateral incisor segment about 40 %, and the lateral‑to‑canine segment about 30 %. This proportion helps achieve a harmonious, natural‑looking smile.
3D‑printed resin veneers have demonstrated impressive durability. Clinical data show that these digitally fabricated restorations typically survive five years or more, maintaining colour stability and resistance to wear. When minor chipping or staining occurs, touch‑ups or re‑polishing can extend their functional life without full replacement.
Looking ahead, guided implant surgery is being reshaped by emerging technologies. Artificial‑intelligence‑driven treatment planning can automate prosthetically driven implant placement, reducing human error. Augmented‑reality headsets overlay the virtual plan onto the patient’s anatomy, offering real‑time navigation that rivals static guides. Finally, robotic systems are beginning to integrate with AI and AR, delivering sub‑millimetre positional accuracy and consistent angular control, which may become the new gold standard for complex cases.
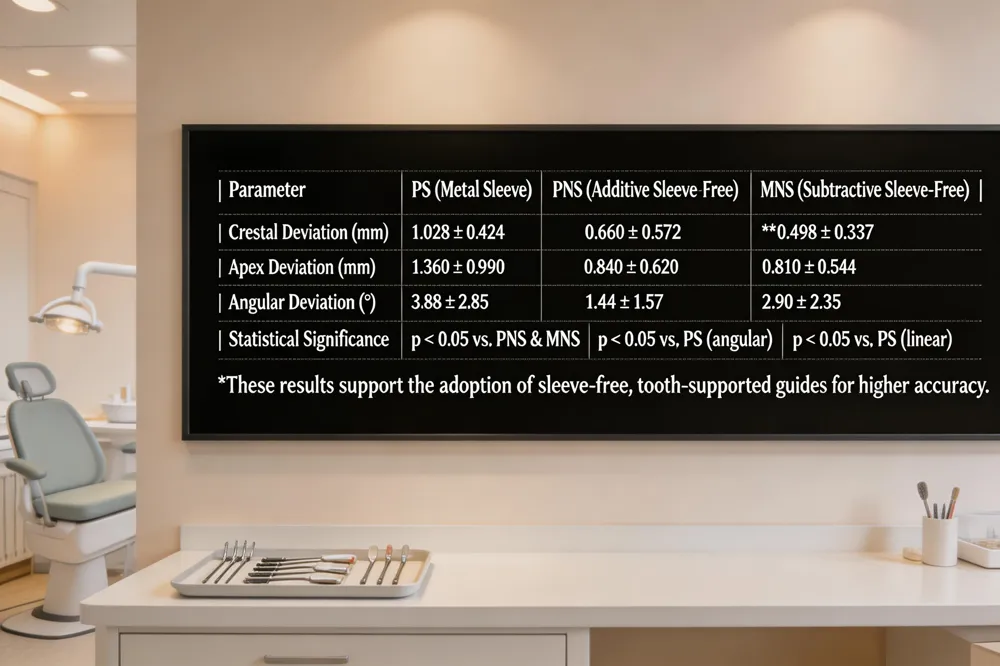 An in‑vitro study placed 72 implants in 12 dentally supported, 3‑D‑printed maxillary models using three guide designs: additive‑manufactured with metal sleeves (PS), additive without sleeves (PNS), and subtractive milled without sleeves (MNS). All guides were anchored with two pins and employed a standardized 4.85 mm internal drill diameter. Statistical analysis (Kruskal‑Wallis and Mann‑Whitney, p < 0.05) showed that sleeve‑free guides (PNS and MNS) significantly outperformed the metal‑sleeve PS guide for every accuracy parameter. The MNS group achieved the smallest mean crestal deviation (0.498 ± 0.337 mm) and apex deviation (0.810 ± 0.544 mm), while the PNS group exhibited the lowest angular deviation (1.44° ± 1.57°), better than both MNS (2.90° ± 2.35°) and PS (3.88° ± 2.85°). For Gentle Dentistry’s chair‑side workflow, these findings support the adoption of 3‑D‑printed, sleeve‑free, tooth‑supported guides—particularly additive‑printed designs—to minimize positional errors, shorten surgical time, and enhance patient safety while maintaining cost‑effective, in‑office production.
Recent studies consistently show that static, 3D‑printed surgical guides reduce implant placement errors to sub‑millimetre levels and angular deviations to 2–3°. Sleeve‑free, additive‑manufactured guides achieve the lowest crestal and apical deviations, while additive guides without metal sleeves provide the best angular control. Gentle Dentistry of Staten Island adopts an in‑house digital workflow: intra‑oral scanning, CBCT merging, virtual planning, and DLP printing of biocompatible resin guides that are autoclaved and seated on the patient’s dentition with anchor pins. This chairside process shortens surgical time, eliminates flap‑raising, and ensures reproducible accuracy even for less‑experienced clinicians. Patients benefit from reduced chair time, minimized postoperative discomfort, and higher confidence in predictable prosthetic outcomes. Looking ahead, integration of AI‑driven planning and dynamic navigation promises even greater precision and personalized care for future dental practice worldwide.



